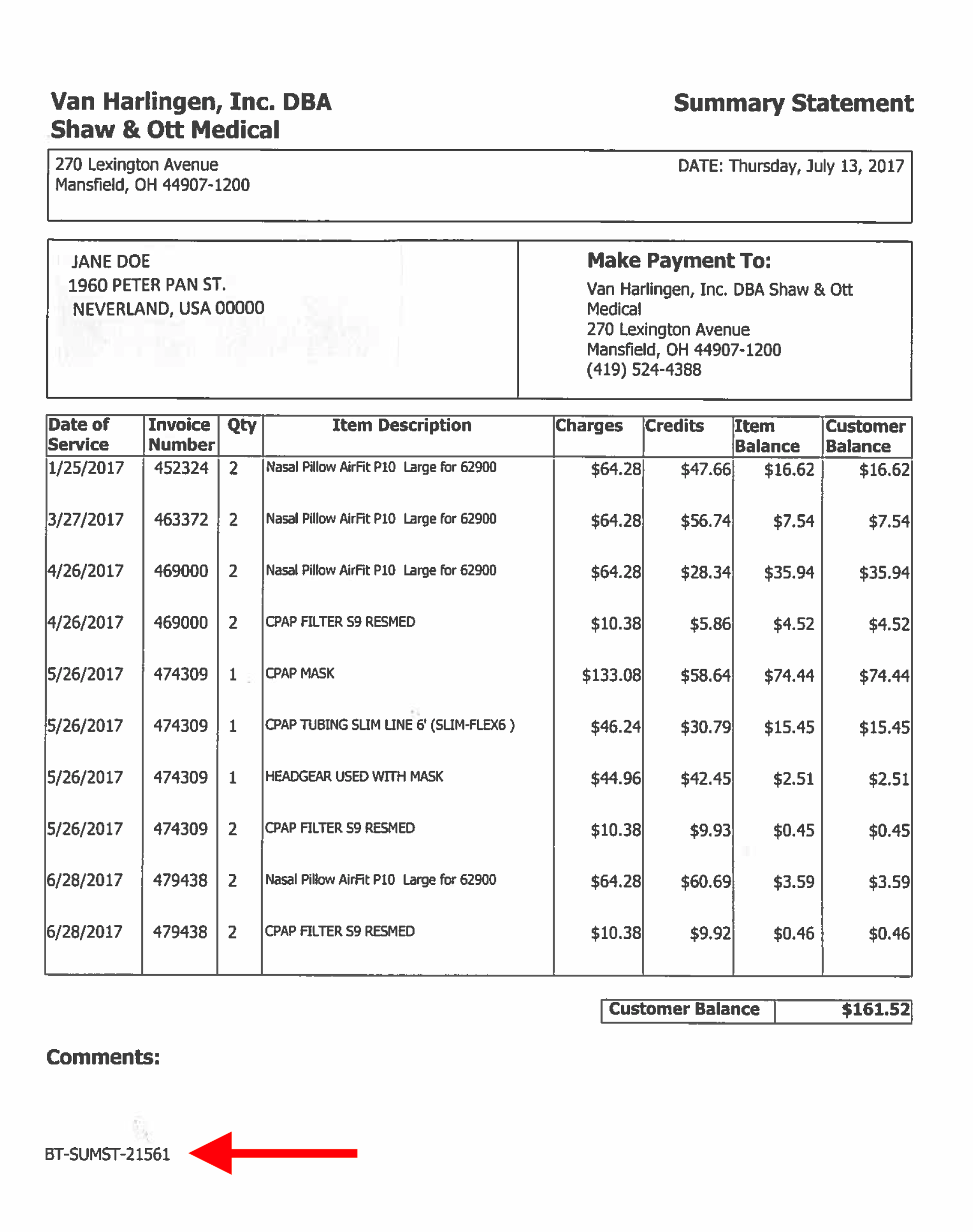
"*" indicates required fields Patient Name* First Last Email* Phone*Statement ID* Payment Amount* Credit CardCard Details Cardholder Name Total EmailThis field is for validation purposes and should be left unchanged.